 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Vamsi Reddy1*, Nitish Sood1, Jennifer Hua2 and Christ opher Ibikunle3
1Medical College of Georgia, Augusta University, Georgia, United States
2Georgia Campus, Philadelphia College of Osteopathic Medicine, Pennsylvania, United States
3Georgia SurgiCare, Ideal Body Institute, United States
*Corresponding author: Vamsi Reddy, Medical College of Georgia, Augusta University, Georgia, United States, E-mail: VAREDDY@augusta.edu
Received: December 26, 2019; Accepted: Janurary 05, 2020; Published: Janurary 11, 2020
Citation: Reddy V, Sood N, Hua J et al. (2020) A Retrospective Analysis of Weight Loss Associated with the ORBERA Intragastric Balloon at a Single Bariatric Center. J Med Res Surg 1(1): 1-3.
Copyright: © 2020 Reddy V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Retrospective Study: An assessment of weight loss and safety profile of ORBERA Intragastric Balloon System (IBS).
Background: Lifestyle modification and dietary management have proven to be ineffective in the treatment of obesity. ORBERA Intragastric Balloon (IGB) system, a treatment modality approved by the US Food and Drug Administration has recently become available commercially for the treatment of refractory obesity in patients with Body Mass Index (BMI) of 35-40. Setting: A private clinic based in the United States.
Objectives: Data on the effectiveness and accommodative adverse effect of ORBERA IGB are currently limited. The objective of this study is to measure the effect of IGB on weight loss, assess the accommodative adverse event safety profile and examine factors associated with accommodative symptoms such as nausea and vomiting.
Methods: A review of records of 22 patients treated using ORBERA in a private clinic from September 2016 to January 2018 was conducted. The balloons were filled with 400-600 mL of saline solution. The IGB was placed and removed endoscopically over a treatment period of 6 months.
Results: The sample size comprised of 18 (81.82%) females and 4 (18.18%) males with a mean age of 49.23 (range 21-76 years). The most common comorbidities in this population were gastroparesis (4, 20%), hiatal hernia (6%29%), diabetes mellitus (3%-15%), and cholecystitis (2%-10%). The baseline mean weight was 239.26 lb (range 158 lb-323 lb), baseline mean BMI was 39.48 (range 29.85-48.90).The mean end of treatment weight was 182.2lb (range 134 lb-279 lb) with a mean weight loss of 32.2 lb (range 16 lb-48 lb) and a mean BMI 30.79 (range 25.3- 40.2) at end of the 6 months treatment period. No serious adverse events were observed during the endoscopic placement and removal of the system. The most frequent accommodative adverse events were nausea 13 (65%), vomiting 12 (60%), reflux/Gastroesophageal reflux disease 8 (40%). No significant characteristics associated with the accommodative side effects (e.g. nausea and vomiting) were discernible.
Conclusion: The findings suggest that ORBERA IGB is an effective, safe and reasonably well-tolerated management option for obesity as significant weight loss was found consistently in the study population. However, further study is recommended for a better understanding of the accommodative symptoms associated with the IGB system.
Weight loss; Bariatric center; Orbera intragastric balloons; Gastroesophageal; Bariatric surgery
Obesity is a global epidemic one that no country has been able to tackle effectively [1]. In the United States, obesity rates have been increasing since the 1980s [2]. The prevalence of obesity in adults over the age of 20 has steadily risen over the last decade, reaching 39.8% in 2017 [2]. This is estimated to reach approximately 42%-51% by 2030 [3,4]. Even a one percent decrease from this predicted value would correlate with a $4.0 (± $0.5) billion reduction in obesity-attributable medical spending by 2020 [5]. Thus highlighting the importance of finding sol tions to this epidemic.
Additionally, obesity’s link with decreased life expectancy is wellestablished. A prospective cohort study with over 60,000 participants found that among non-smokers at age 50, obese populations have a two to three-fold increase in mortality risk when compared to non-obese populations [5]. Traditional weight loss goals aim for a five to ten percent decrease in body weight which has been shown to slow the onset of obesity-related co-morbidities such as type 2 diabetes (T2D) [6,7] As the population of obese individuals in the United States continues to grow, it becomes increasingly important to evaluate the different treatment options and their roles in patient care. Physical exercise, energy-restricted diets, and behavior modification remain the first-line treatment options for almost all patients. These play a critical role in not only treatment but also prevention [8]. Pharmacotherapy is often used as a secondary option for patients in whom lifestyle changes have been unsuccessful. Surgical alternatives, including adjustable gastric banding and gastric bypass procedures, have long been demonstrated to be more effective at inducing weight loss in patients who are severely obese [9]. Despite the proven efficacy of bariatric surgery, very few eligible candidates with morbid obesity choose to undergo surgical weight-loss procedures [9,10]. Many prospective patients have shied away from surgical options due to fear of invasive procedures and potential complications;6 for this group, endoscopic alternatives may appear more attractive. Additional market segments include severely ill patients who are poor surgical candidates as well as very obese patients (Body Mass Index (BMI)>40 kg/m2 or BMI>35 kg/m2 with obesity-associated comorbidities) for whom a moderate preoperative weight loss may reduce surgical complications [6,11]. We present a retrospective study of 22 patients with BMIs ranging from 30 to 49 who underwent endoscopic placement of Orbera Intragastric Balloons (IGB). .
A review was conducted of the 22 patient records for those undergoing placement of the Orbera Intragastric Balloon between September 2016 to January 2018. No super-obese patients were included (BMI>50 kg/m2) within the study. All had previously failed to achieve desired levels of weight loss using traditional weight control programs. The IGBs were filled with 400 mL-600 mL of saline solution. For each patient, the IGBs were placed and removed endoscopically after a treatment period of six months.
The sample size comprised of 18 (81.82%) females and 4 (18.18%) males with a mean age of 49.23 (range 21-76 years). The most common comorbidities in this population were gastroparesis (4,20%), hiatal hernia (6,29%), diabetes mellitus (3,15%), and cholecystitis (2,10%). Baseline mean weight was 239.26 lb (range 158 lb-323 lb). The mean weight loss was 32.2 (range 16 lb-48 lb), with a mean end of treatment weight of 207.06 lb. Weight loss changes are represented in Figure 1. The baseline mean BMI was 39.48 lb (range 29.85 kg/m2-42.24 kg/ m2). The mean BMI decrease was 5.31 kg/m2, with a mean end of treatment BMI of 34.17 kg/m2. This represents a 13.5% drop in weight over the 6-month treatment period. BMI changes are illustrated in Figure 2.
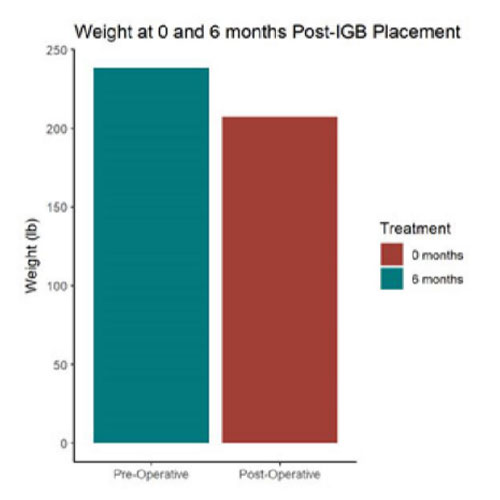 Figure 1: Drop in weight at time points 0 months and 6 months
after ORBERA IGB placement.
Figure 1: Drop in weight at time points 0 months and 6 months
after ORBERA IGB placement.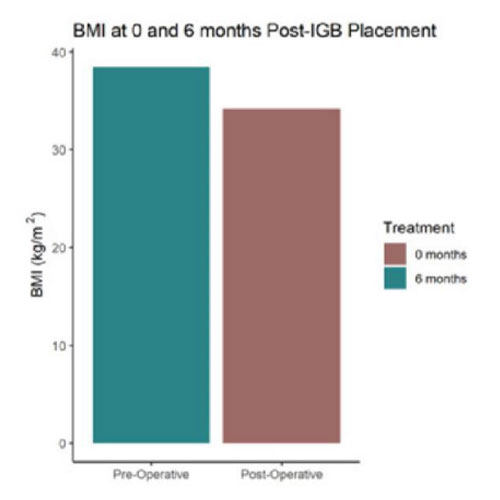 Figure 2: Drop in BMI at time points 0 months and 6 months after
ORBERA IGB placement.
Figure 2: Drop in BMI at time points 0 months and 6 months after
ORBERA IGB placement.
Treatment with Orbera Intragastric Balloon coupled with changes in diet and exercise-induced an average weight loss of 13.5%. This difference was not statistically significant across different ages or genders and represented a slightly greater decrease in weight than that found in a recent meta-analysis. Significant weight loss was consistently found within the study population. Overall, this suggests Orbera IGB is an effective, safe, and well-tolerated management option for obesity. However, further study is recommended for a better understanding of the accommodative symptoms associated with the IGB system.
onflict of Interest We declare that there is no conflict of interest regarding the publication of this paper.

